What is it ?
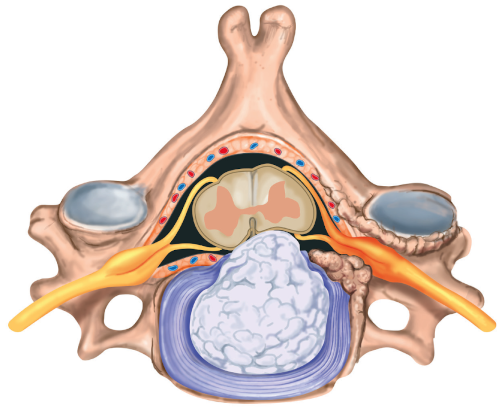
Cervical disc herniation is defined as a part of the intervertebral disc pushing into the cervical spinal canal: protrusion, fragment, etc. The natural aging of the disc causes its dehydration. The disc therefore becomes less effective mechanically, but it can also fragment and push back into the cervical spinal canal. The picture below represents a cervical disc herniation: the fibrous annulus can be seen (in blue), with a part of the disc nucleus protruding into the spinal canal.